
min. read
Topics
For select patients with severe congenital diaphragmatic hernia (CDH), we offer fetal endoscopic tracheal occlusion (FETO), a breakthrough procedure with the potential to help improve lung growth before birth. Fetal endoscopic tracheal occlusion (FETO) is also sometimes referred to as fetoscopic endotracheal occlusion or fetoscopic endoluminal tracheal occlusion.
Texas Children’s is one of the few fetal centers in the nation to offer FETO, a minimally invasive procedure that involves inserting a tiny balloon into the fetus’ trachea. The procedure is performed by one of the most skilled and experienced teams of physicians in the use of this experimental treatment.
What is Congenital Diaphragmatic Hernia?
Congenital diaphragmatic hernia (CDH) is a hole in the baby’s diaphragm, the muscle that separates the abdomen from the chest. This opening allows abdominal organs (stomach, intestine, liver and spleen) to move up into the fetal chest cavity, crowding the lungs and preventing them from developing normally.
Babies with CDH often have small, underdeveloped lungs, known as pulmonary hypoplasia, leading to breathing problems at birth.
About the Procedure
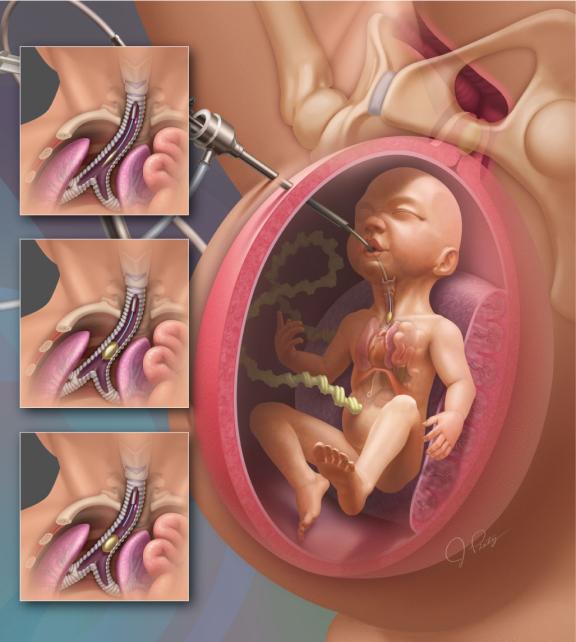
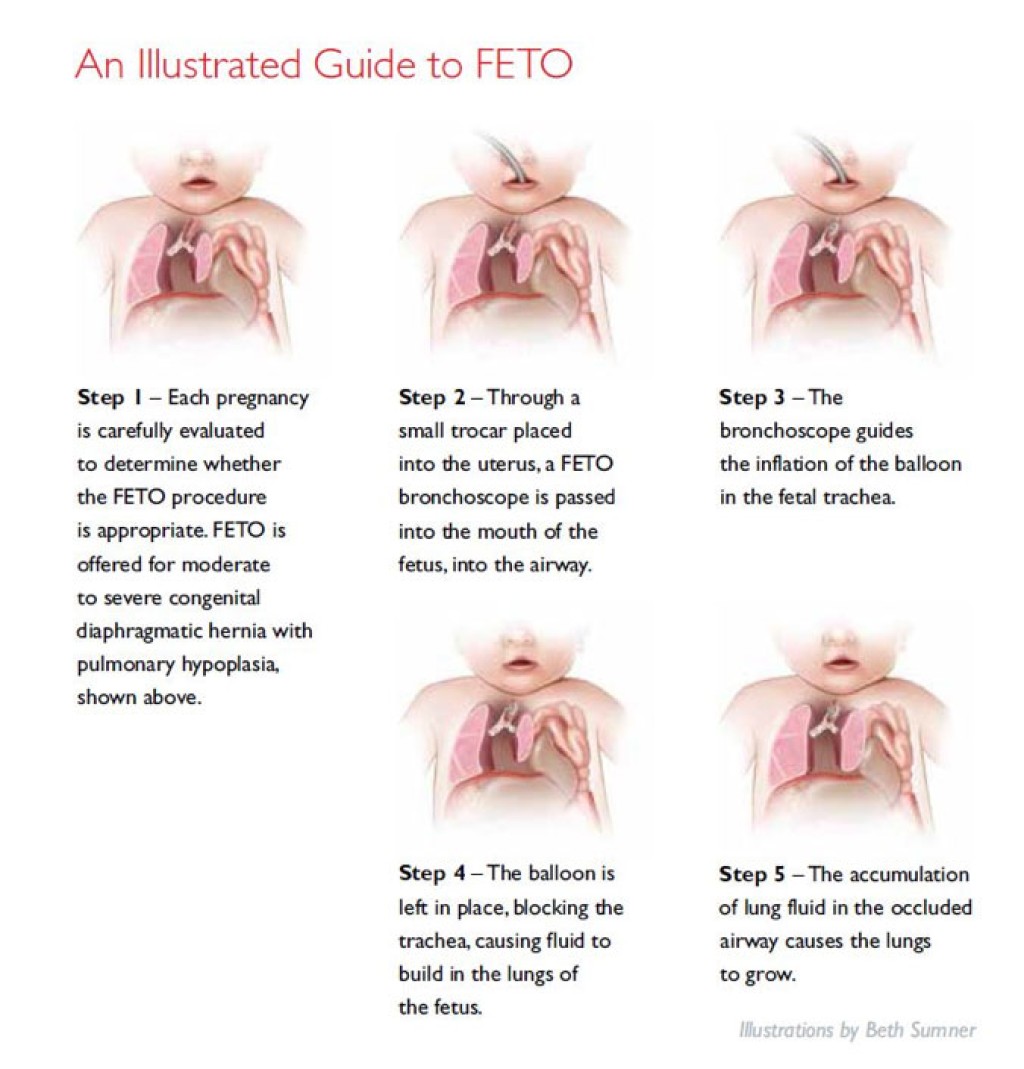
FETO is performed between 26 and 28 weeks of gestation. During the procedure, the mother and fetus are sedated, and the mother is given medication to help prevent labor.
A tiny incision is made in the mother’s abdomen and uterus. Guided by ultrasound, the surgeon inserts a tube about the size of a straw, known as a “trocar.” The surgeon then inserts an endoscope, a tiny tube with a camera on the tip, through the trocar, into the mouth of the fetus and into the trachea. A small balloon is placed inside the trachea and inflated, blocking the airway to promote lung growth. The fetus will continue to receive oxygen through the placenta.
The balloon is removed through a second procedure prior to the baby’s birth, typically around 34 weeks of pregnancy.
How does blocking the trachea improve fetal lung growth?
The fetal lungs make fluid throughout the pregnancy. This fluid exits the lungs through the trachea and goes out into the amniotic fluid.
When the trachea is blocked by the balloon, the fluid builds up and inflates the underdeveloped lungs, stimulating their growth.
Risks
As with any surgical intervention, FETO has risks. These risks include:
- Preterm labor
- Loss of pregnancy
- 30% risk of membrane rupture (rupture of the amniotic sac resulting in preterm delivery)
Talk with your doctor about these risks to help you and your family decide if the benefits of FETO outweigh the potential complications.
After the Procedure
After surgery, mother and baby will be closely monitored throughout the remainder of the pregnancy with weekly ultrasounds.
Because the FETO procedure temporarily blocks the baby’s airway, it is imperative that the mother remain within 30 minutes of the fetal center while the balloon is in place, ensuring immediate access to specialized care in case of an emergency delivery.
At Texas Children’s, our FETO team is on standby 24/7 should mother and baby need us. Your family will meet with one of our social workers, who will assist you with your stay in Houston.
At around 34 weeks of pregnancy, a second procedure will be performed to remove or deflate the balloon prior to birth. The baby’s lungs can then continue to develop throughout the remainder of the pregnancy. This procedure does not increase the risk for cesarean section.
Surgery to close the hole in the baby’s diaphragm is typically performed after birth, once the newborn is stable.
Is my baby a candidate for FETO?
FETO may be an option for severe cases of CDH, where the fetal lungs are extremely small and, despite the best medical care and treatments available, the child may not survive after birth.
Mothers considering FETO should be examined in our fetal center as early as possible after diagnosis of congenital diaphragmatic hernia, preferably between 22 and 26 weeks gestation. Our experienced specialists will conduct a thorough evaluation, including an ultrasound, fetal echocardiogram and amniocentesis, and make treatment recommendations based on your baby’s unique condition.
Volumes and Outcomes
Our outcomes in FETO and CDH repair are among the best in the country.
- View data on our experience and outcomes of FETO (fetal endoscopic tracheal occlusion)
- View data on our experience and outcomes treating congenital diaphragmatic hernia (CDH)
Read the most recent study showing outcomes of FETO for fetuses with severe cases of CDH:
Why Texas Children’s Fetal Center?
Texas Children’s Fetal Center is one of the oldest and most experienced programs in the nation. We have a history of leading the development and implementation of innovative fetal therapies and procedures such as FETO, offering families new options for the treatment of severe CDH and other fetal anomalies.
Here, you and your baby will receive expert maternal, fetal and pediatric care for congenital diaphragmatic hernia all in one location. Our multidisciplinary team includes some of the nation’s top maternal-fetal medicine specialists, surgeons, neonatologists, pediatric cardiologists and pulmonologists, among others.
24736
Conditions
article