
min. read
Pierre-Robin Sequence (PRS) is a condition where babies are born with a small lower jaw (mandible), causing their tongue to obstruct their airway, especially when they are sleeping on their back (Figure 1). The majority, but not all, of children with PRS also have a cleft palate. Because of airway obstruction, babies with PRS may also have difficulty feeding. Newborns with PRS require close attention, and care by a multidisciplinary team of experts at a craniofacial center.
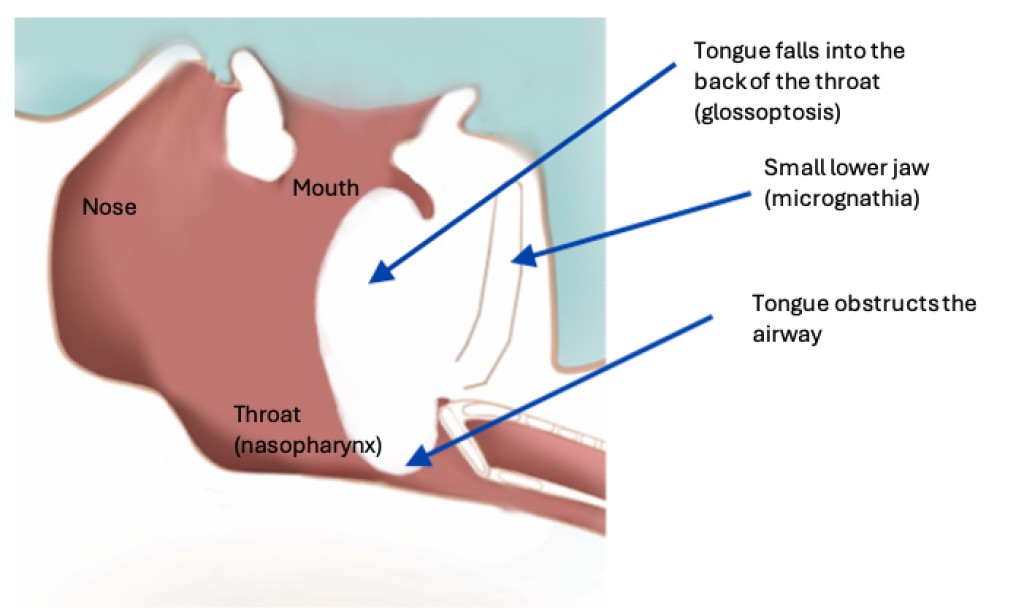
Figure 1: Side view of a baby with Pierre-Robin sequence lying on his/her back. The baby exhibits a small lower jaw (micrognathia), and a tongue that falls into the back of the throat (glossoptosis), causing airway obstruction
The immediate treatment of babies with PRS focuses on ensuring that their airway is stable, and that they are receiving enough calories to grow.
Airway treatment: Initial conservative measures to treat the airway include positioning the baby in a side-lying position or a prone position to sleep. This uses gravity to pull the tongue forward and out of the airway. In some babies with severe airway obstruction, immediate intubation may be necessary.
Some children with PRS have additional airway abnormalities that may also cause obstruction. These may include laryngomalacia (floppy larynx or voicebox), tracheomalacia (floppy trachea or windpipe), or others. Therefore, an endoscopy to examine the entire airway is usually needed.
When able, a polysomnogram (sleep study) should be obtained. This helps determine what type of sleep apnea the baby has, and how severe it is. The polysomnogram can also help determine whether side or prone positioning are helpful to treat the obstruction.
Children with PRS should be seen by multiple specialists. These include a craniofacial plastic surgeon, an otolaryngologist, a feeding therapist, a sleep pulmonologist, a geneticist, and potentially a neonatal intensive care physician.
Depending on the results of the workup, babies with PRS may be continued on positioning treatment if their airway is stable. Alternatively, they may require mandibular distraction osteogenesis (MDO). In a small number of children, especially those who have airway obstruction at multiple levels, a tracheostomy may be necessary.
Feeding: It is important to make sure that babies with PRS are receiving enough calories and gaining weight appropriately. Airway obstruction can make it difficult to feed. In addition, babies with PRS may need to work extra hard to breathe, which causes them to burn more calories, which then impairs their ability to gain weight. Most babies with PRS initially require a feeding tube that goes from their nose into their stomach. With time, and as the airway obstruction is treated, feeding may improve to the point where the baby is able to gain weight by eating orally, and the feeding tube may be able to be removed. In some babies, a feeding tube may be needed for a longer time period, and a gastrostomy tube (G-tube) may be placed.
75926
Conditions
article