
min. lectura
Temas
What is an anorectal malformation or an imperforate anus?
Anorectal malformation, also known as imperforate anus, is a condition with which children are born with an abnormal anal opening. This condition affects 1 in 5,000 children. The causes of this condition are not known for sure, but are likely due to a problems with prenatal development of the digestive tract.
Types
Image
Image
Perineal fistula: The rectum inserts onto the perineum and may be partially or completely outside the muscle complex. The opening is typically smaller than a normal rectum. A sub-epithelial tract with small beads of meconium (baby stool) may be present.
Image
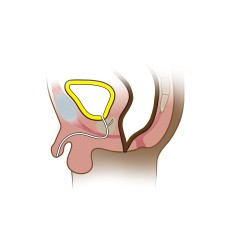
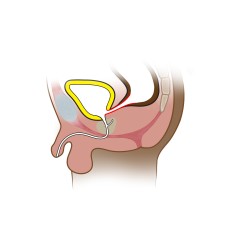
Recovestibular fistula: The rectum inserts into the vestibule, which is the entrance of the vagina.
Image
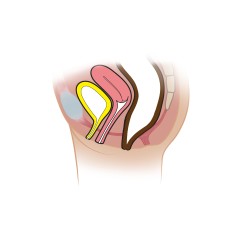
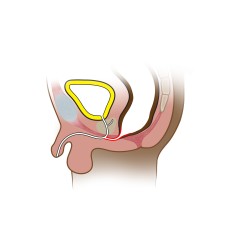
Rectovaginal fistula: The rectum inserts into the posterior wall of the vagina. This maybe in a low or high position on the vagina, which can affect how the procedure is performed. If it inserts high onto the vagina, it may need to be approached from the abdomen.
Image
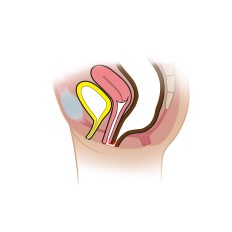
Rectobulbar urethral fistula: The rectum inserts onto the bulbar portion of the urethra, which is a more distal portion of urethra and can usually be reached from a posterior approach.
Image

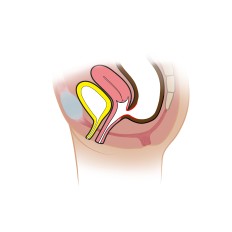
Rectoprostatic urethral fistula: The rectum inserts on the prostatic portion of the urethra. This maybe reach from a posterior or abdominal apporach.
Image
Rectobladder neck fistula: The rectum inserts onto the bladder neck, which is above the urinary sphincter mechanism. This is usually approached from the abdomen.
Anorectal malformation without fistula: The rectum is blind-ending and does not connect to either the urethra or vagina.
Anal stenosis: The anus is within the sphincter complex but is smaller than a normal rectum. The anus may appear “funnel-shaped.” This condition may be associated with other sacral anomalies or a prescral mass called Currarino’s triad.
Diagnosis
Most anorectal malformations are detected shortly after birth. There may be a small anal opening or no opening at all. Patients with anorectal malformations often have other congenital anomalies, which are called “VACTERL syndrome,” and should be screened for these other conditions.
Treatment
Depending on the type of malformation, your team may recommend a colostomy first. A colostomy is a procedure when the colon is brought up to the abdominal wall and the stool goes into a bag instead of through the anus. This is typically done when there is no anal opening on the perineum or vestibule or if your child has other severe anomalies.
If your child has a perineal or vestibular fistula, your team may recommend surgical correction within the first several months of life. Babies are typically sent home with dilations prior to repair.
The procedure used to fix most anorectal malformations is called a Posterior Sagittal Anorectoplasty (PSARP). The surgeon will use a nerve stimulator device to locate the sphincter muscles. An incision is then made down the midline to split the muscles. The rectum is dissected free and placed within the muscle complex.
If your child’s anorectal malformation needs to be approached from the abdomen, your surgeons will often use a technique called a Laparoscopic Assisted Anorectoplasty (LAARP). This procedure involves mobilization of the rectum and division of the fistula using a camera and small incisions. The sphincter muscles are identified in a similar fashion to the PSARP and an incision made between them. The rectum is brought through this incision and placed within the muscles
If your child has a colostomy, it may be reversed several months after the PSARP or LAARP. Your provider will discuss whether or not dilations are necessary after surgery. Most surgeons no longer require dilations after surgery and will instead perform a small procedure called a stricturoplasty at the time of colostomy reversal to widen the anoplasty.
23951
Conditions
article