min. read
Topics
Double outlet right ventricle (DORV) is a congenital heart defect, meaning it is present at birth. It occurs when the heart doesn’t form properly during fetal development. In most cases, the cause is unknown.
DORV is a complex abnormality that has many variations and typically involves other heart defects as well.
What happens in DORV?
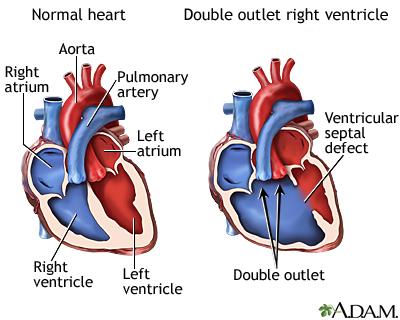
There are two main arteries that carry blood out of the heart: the aorta and the pulmonary artery, also known as the “great vessels.”
In a normal heart:
- The aorta is connected to the left ventricle, the chamber of the heart that pumps red, oxygen-rich blood out into the body
- The pulmonary artery is connected to the right ventricle, the chamber of the heart that pumps blue, oxygen-poor blood to the lungs
In babies with DORV, both the aorta and pulmonary artery are connected to the right ventricle.
A.D.A.M Interactive Anatomy®
In addition, almost all babies with DORV also have a ventricular septal defect (VSD), an abnormal opening in the wall between the left and right ventricles that allows blood from each side of the heart – oxygen-rich and oxygen-poor blood – to mix together.
For babies with DORV, this hole is helpful, providing the only way for oxygenated blood to reach the right ventricle, where the aorta is connected, and be pumped out into the body.
However, because the blood is mixed, it is not as high in oxygen as it should be.
Risks to the Baby
In babies with DORV, the heart has to work harder than normal to pump enough oxygenated blood out into the body, which can cause the heart to become enlarged. Too much blood may also be pumped to the baby’s lungs.
Without treatment, risks include high blood pressure and heart failure.
Types of Ventricular Septal Defects (VSDs)
There are four types of ventricular septal defects that occur in DORV, based on where the opening is located:
- A subaortic VSD is located below the aorta, allowing oxygen-rich blood to flow from the left ventricle, through the VSD, and into the aorta. Blood from the right ventricle flows mainly into the pulmonary artery.
- A subpulmonary VSD is located below the pulmonary artery, a condition known as a Taussig-Bing anomaly. Oxygen-rich blood flows from the left ventricle, through the VSD, and into the pulmonary artery. Oxygen-poor blood from the right ventricle flows mainly into the aorta.
- A doubly committed VSD means there are two VSDs, one below the aorta and one below the pulmonary artery.
- A remote (non-committed) VSD means the hole is not near the aorta or the pulmonary artery.
Types of DORV
DORV differs in each baby based on the location of the VSD, the positioning of the aorta and pulmonary artery (which are normally side-by-side), and other cardiac defects involved. The impact these variables have on the normal blood flow through the heart will determine the baby’s prognosis and the intervention required.
There are three major types of DORV:
- Tetralogy of Fallot (TOF) – a condition involving four abnormalities occurring together, including narrowing of the pulmonary valve or artery (pulmonary stenosis), decreasing pulmonary blood flow
- Transposition of the Great Arteries (TGA) – when the positioning of the aorta and pulmonary article are switched or “transposed”
- VSD DORV – the most common type of DORV, with pulmonary over-circulation (an increase of blood flow to the lungs) and no outflow tract obstruction
Risk Factors
DORV occurs in an estimated 6 to 15 infants per 100,000 live births. It is more common in males.
Babies with certain genetic abnormalities are at increased risk for double outlet right ventricle, including trisomy 13 and trisomy 18.
Genetic counseling and testing is recommended for all women pregnant with a baby with DORV.
Symptoms
Newborns with DORV typically show signs of the condition within a few days of birth.
While the signs and symptoms can vary for each baby, in general they may include:
- Rapid breathing or difficulty breathing
- Heart murmur
- Rapid heartbeat
- Sweating
- Extreme tiredness
- A blue tint to the skin, lips or nails (cyanosis), due to lack of oxygen in the blood
- No interest in feeding
- Weight loss or poor weight gain
Diagnosis
During Pregnancy
Double outlet right ventricle may be detected before birth during a routine prenatal ultrasound. Your OB/GYN will refer you to a pediatric cardiologist, who will perform a fetal echocardiogram (cardiac ultrasound) to better view and evaluate your baby’s heart structure and blood flow.
You and your baby will be monitored closely throughout your pregnancy. Your care team will include maternal-fetal medicine specialists, pediatric cardiac surgeons, pediatric cardiologists, and neonatologists, for a well-planned, well-coordinated approach to prenatal care, delivery and treatment after birth.
After Birth
In other cases, DORV may not be detected until the baby is born and shows signs and symptoms such as breathing problems, a blue tint to their skin, or a heart murmur, the sound of blood moving abnormally through the heart.
Tests to confirm the diagnosis may include:
- Pulse oximetry, to measure the oxygen level in the baby’s flow
- Chest X-ray
- Electrocardiogram (ECG or EKG), to measure the heart’s electrical activity
- Echocardiogram, to view the heart’s structure and blood flood
- Cardiac MRI or CT scan, for more detailed imaging of the heart
- Cardiac catheterization, to further evaluate the heart and defect
Treatment
Surgery is required to correct double outlet right ventricle, enabling blood to flow normally out of the heart to the body and lungs.
The timing and type of surgery depends on each baby’s defect, other heart abnormalities, and overall health. If symptoms are severe, the surgery may be performed the first few days after birth. In complex cases, a series of surgeries may be required.
Follow-Up Care
Babies born with DORV will need to continue to see a heart specialist throughout their lives, transitioning at adulthood to a cardiologist who specializes in the treatment of adults with congenital heart defects.
Texas Children’s – #1 in the Nation for Pediatric Cardiology and Heart Surgery
Texas Children’s Pavilion for Women and Texas Children’s Fetal Center are nationally recognized centers for the care of fetuses and infants with congenital heart defects, providing mother and baby expert, collaborative care all in one location.
We offer comprehensive fetal cardiac care through our Fetal Cardiology Program, including diagnosis, counseling, delivery planning and seamless transition to treatment at Texas Children’s Heart Center® after birth. Texas Children’s Heart Center is ranked #1 in the nation for pediatric cardiology and heart surgery by U.S. News and World Report.
Volumes and Outcomes
- Texas Children’s Fetal Center Volumes and Outcomes Summary
- DORV patients treated by the Fetal Cardiology program
- Texas Children’s Heart Center Outcomes
Additional Resources
For more information or to schedule an appointment,
call Texas Children’s Fetal Center at 832-822-2229 or 1-877-FetalRx (338-2579) toll-free.
Our phones are answered 24/7. Immediate appointments are often available.
25116
Conditions
article
